Image Gallery
1. An Example of Improper Local Anesthetic Spread
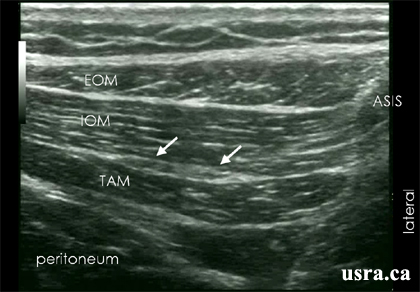
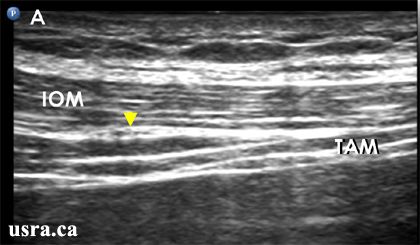
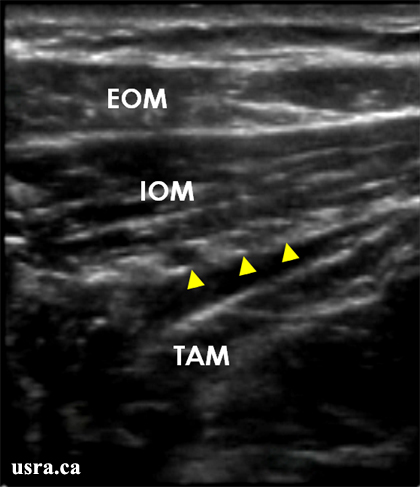
Pre Injection
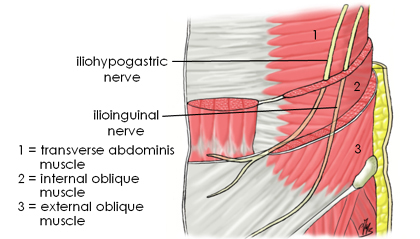
Arrowheads = II/IH nerves in between
EOM = external oblique muscle
IOM = internal oblique muscle
TAM = transverse abdominis muscle
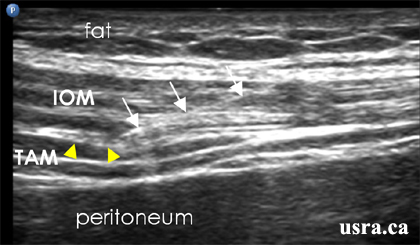
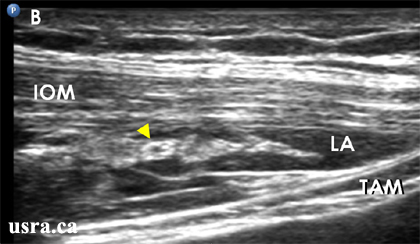
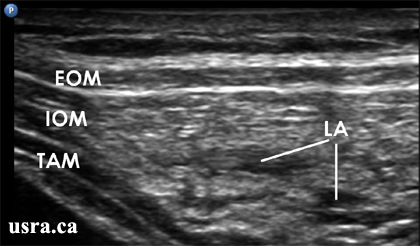
Injection # 1
Local anesthetic (LA) is injected partially within the internal oblique muscle
(IOM) and partially in the plane between the internal oblique muscle and the
transverse abdominis muscle (TAM).
EOM = external oblique muscle
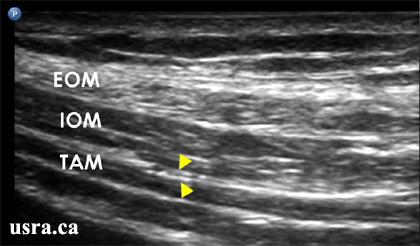
Injection # 2
EOM = external oblique muscle
IOM = internal oblique muscle
TAM = transverse abdominis muscle
An ill defined collection of local anesthetic (LA) is seen around the nerves.
The accuracy of injection is questionable resulting in a partial block.
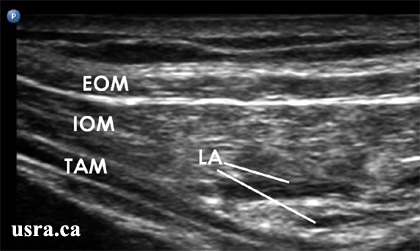
2. Locating A Branch of the Deep Circumflex Iliac Artery
Several hypoechoic structures (arrowheads) may be located within the plane
between the internal oblique muscle (IOM) and the transverse abdominis muscle
(TAM). It is important to use Color Doppler or Color Power Doppler to identify
the branch of the deep circumflex iliac artery (red dot) and not to
inadvertently target the artery.
EOM = external oblique muscle
EOM = external oblique muscle
IOM = internal oblique muscle
Red dot = deep circumflex iliac artery
TAM = transverse abdominis muscle