Scanning Technique
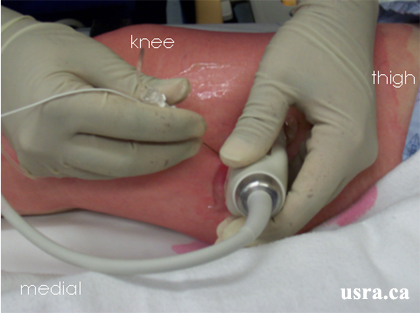
- Position the patient supine with the leg slightly externally rotated.
- Expose the lower part of the thigh, knee and upper leg.
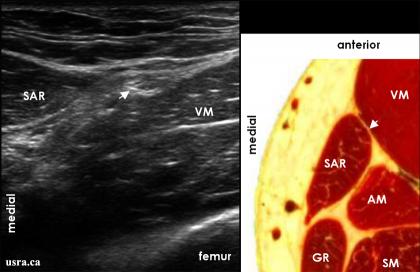
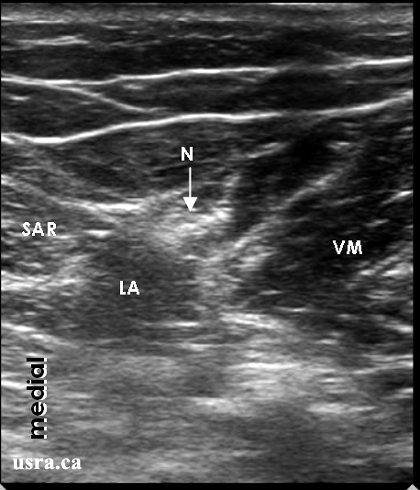
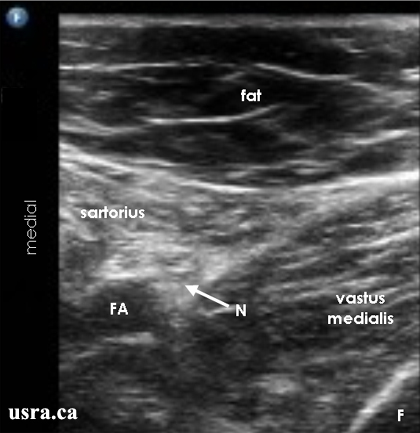
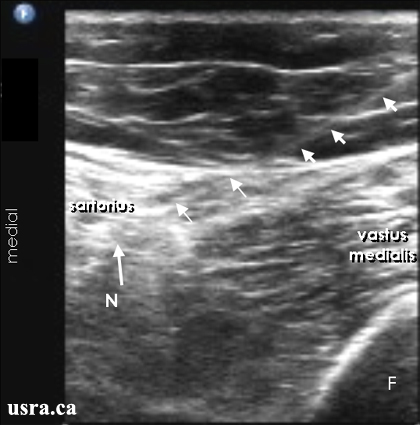
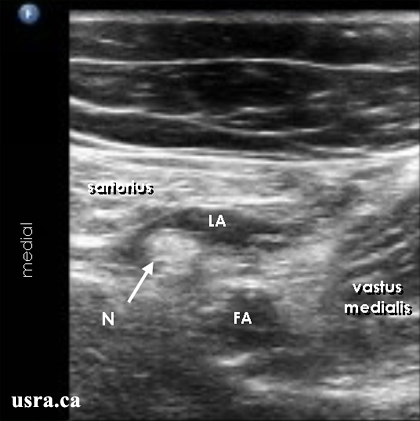
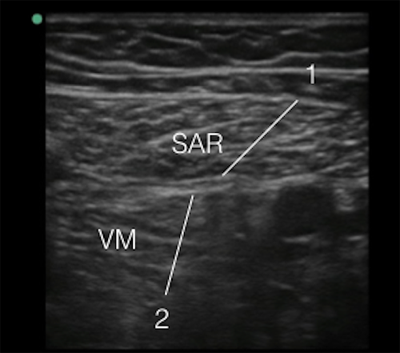
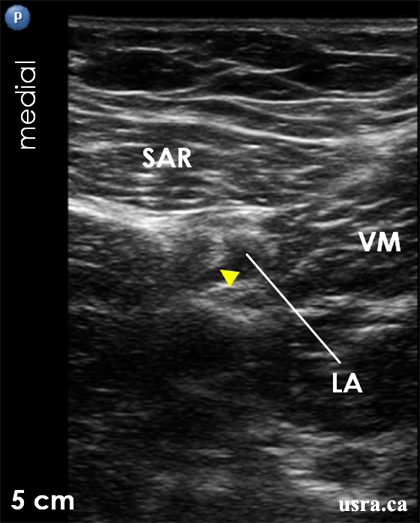
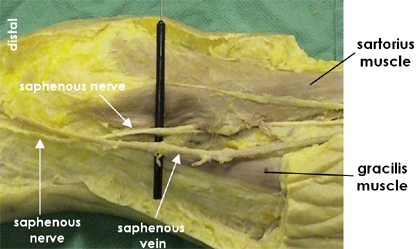
- After skin and transducer preparation, place a linear transducer with the appropriate frequency range (10-12 MHz) starting in the proximal thigh and scan distally to the knee. The saphenous nerve can be blocked reliably in the distal 1/3 of the thigh.
- Optimize machine imaging capability; select appropriate depth of field (usually within 1-3 cm), focus range and gain.

|
Transducer over the medial side of the right thigh. |