Scanning Technique
- Position the patient supine with the leg in the neutral position.
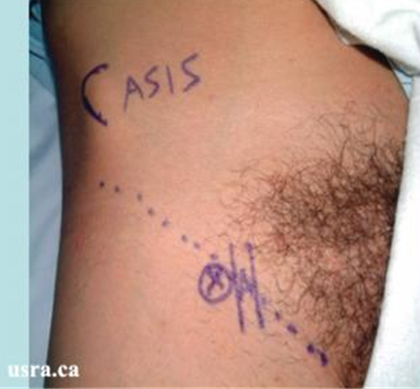
- Expose the groin and mark the inguinal crease.
- After skin and transducer preparation, place a transducer with the appropriate frequency range (10-12 MHz) along the inguinal crease. If the femoral artery and nerve are deep (> 4 cm, use a 7 MHZ transducer).
- Optimize machine imaging capability; select appropriate depth of field (usually within 1-3 cm), focus range and gain.
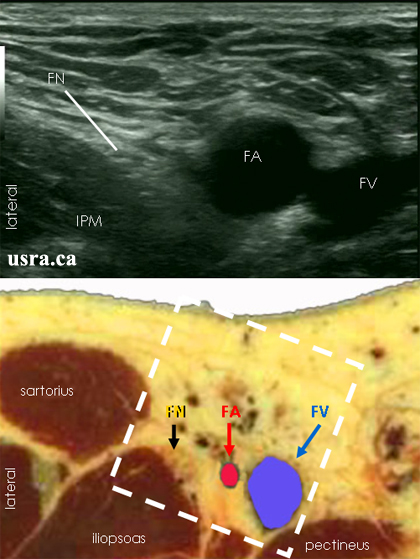
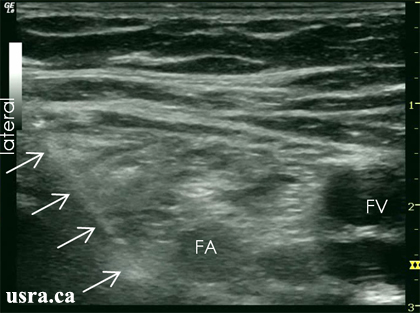
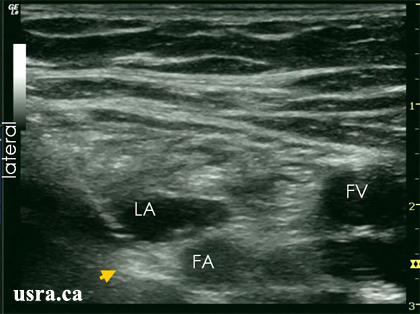
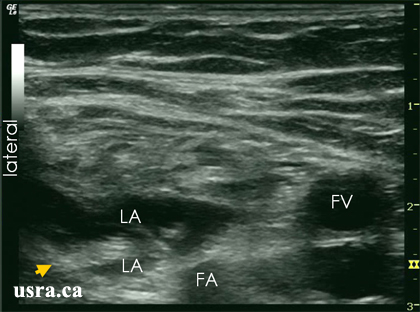
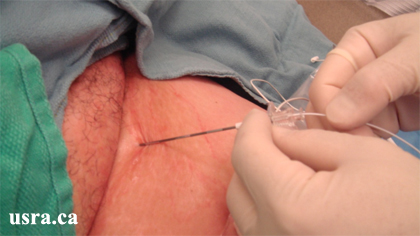
 Transducer over right inguinal crease |
 |