Scanning Technique
- Place the patient in the lateral decubitus position with the side to be blocked uppermost.
- Scan the paravertebral region at L2-3 cephalad to the iliac crest.
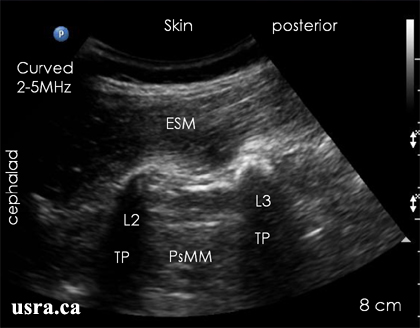
- After skin and transducer preparation, place a curved transducer with the appropriate frequency range (2-5 MHz) longitudinally adjacent to the spine (midline) to capture a longitudinal view of the transverse processes.
- Optimize machine imaging capability; select appropriate depth of field (usually > 8 cm), focus range and gain.
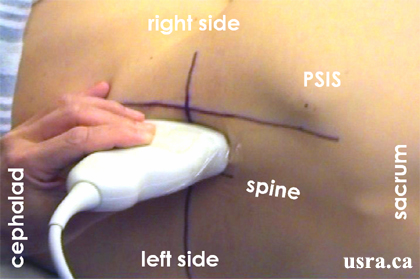
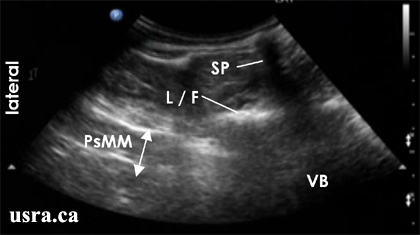
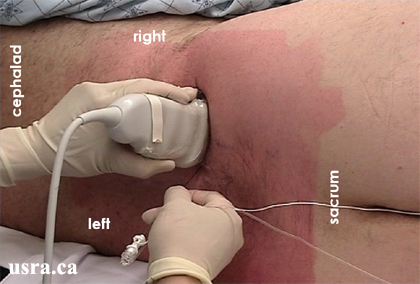
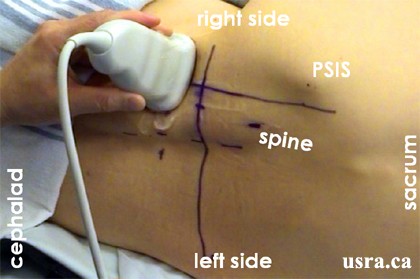
A curved 2-5 MHz transducer over the right paraspinal region to capture a
longitudinal view of the psoas compartment; the patient is in a left
lateral decubitus position
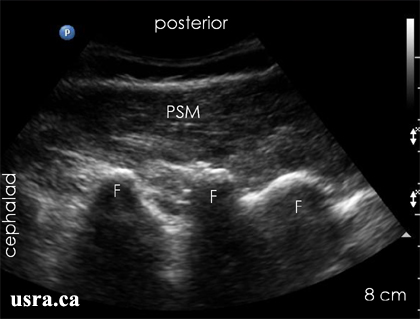
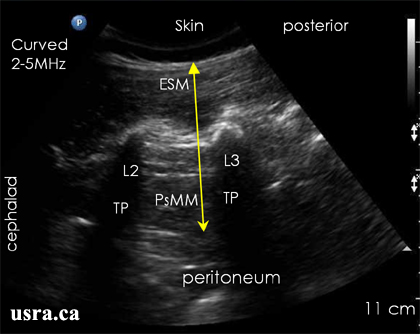
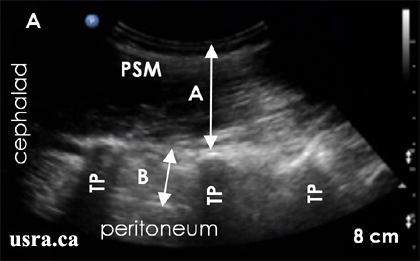
Longitudinal Paravertebral Scan at the L2-3 Level
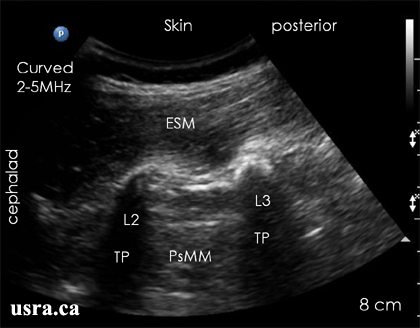
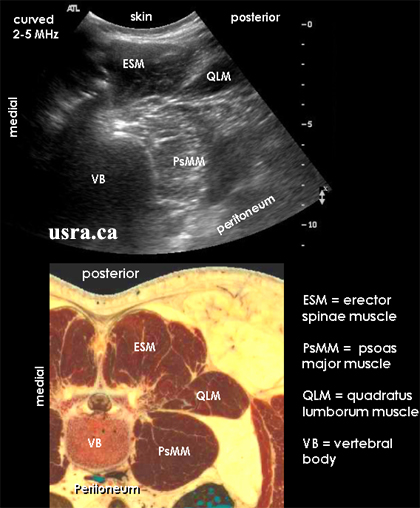
ESM = erector spinae muscle
PsMM = psoas major muscle
TP = transverse processes
PsMM = psoas major muscle
TP = transverse processes
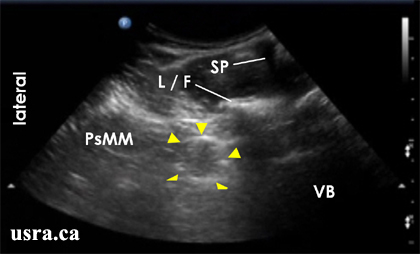
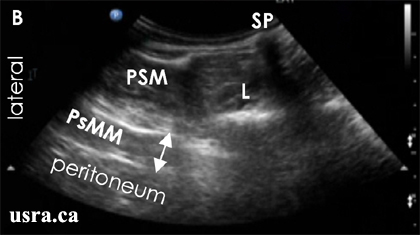
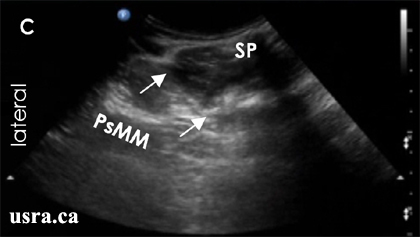
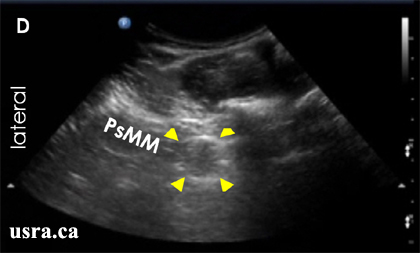
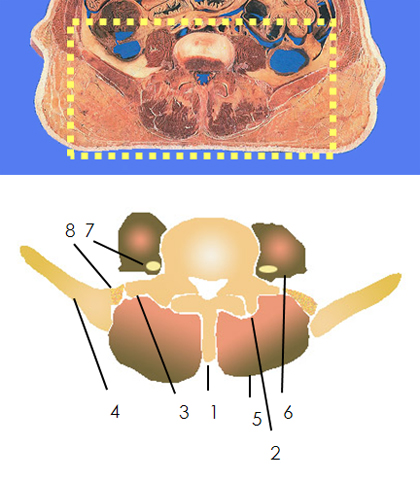
- Turn the transducer transverse to obtain a transverse view of the psoas muscle
- A curved 2-5 MHz transducer over the right paraspinal region to capture a transverse view of the psoas compartment; the patient is in a left lateral decubitus position.