Anatomy
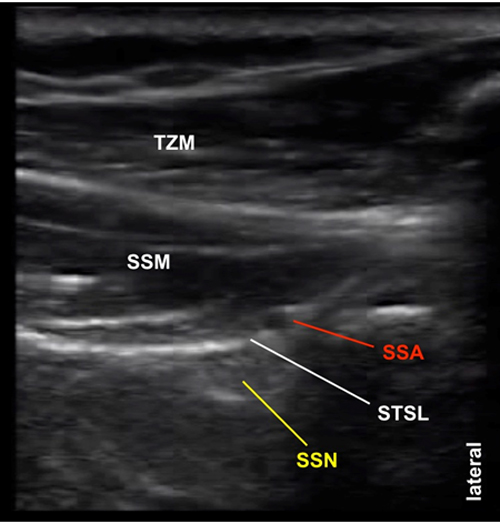
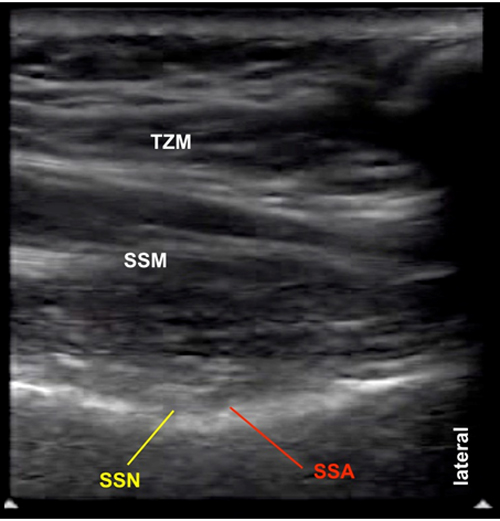
The suprascapular nerve (SSN) is a mixed nerve containing both motor and sensory fibers originating from the superior trunk of the brachial plexus (C5 and C6 nerve roots). Often it receives contribution from the C4 nerve root as well. The SSN passes underneath the omohyoid muscle in the posterior triangle of the neck. Then it passes posteriorly towards the scapula together with the omohyoid muscle towards the suprascapular notch. The nerve passes deep to the superior transverse scapular ligament through the scapular foramen into the supraspinous fossa. At the notch, the nerve is next to the suprascapular artery and vein but the vessels pass above the ligament (Figure 1 and 2).
Figure 1. A schematic diagram showing posterior view of the suprascapular nerve and vessels at the suprascapular notch
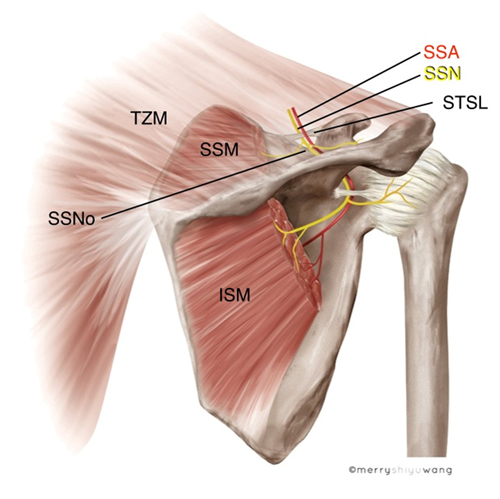 |
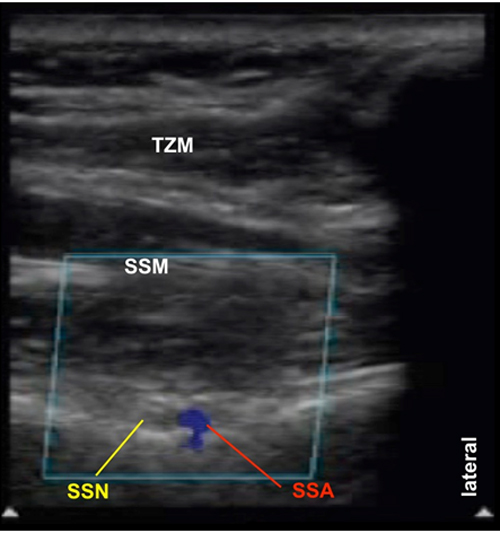
ISM = infraspinatus muscle SSM = supraspinatus muscle SSA = suprascapular artery SSN = suprascapular nerve TZM = trapezius muscle |
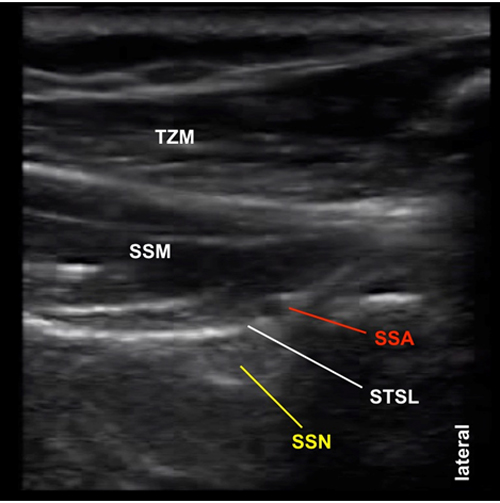
Figure 2. Posterior view of the suprascapular nerve and surrounding structures at the suprascapular notch (cadaver dissection)
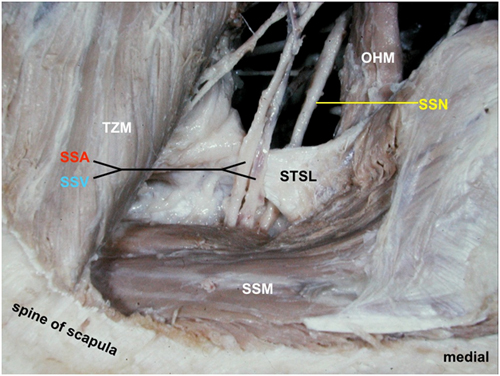 |
OHM = omohyoid muscle SSM = supraspinatus muscle SSA = suprascapular artery SSV = suprascapular vein SSN = suprascapular nerve TZM = trapezius muscle STSL = superior transverse scapular ligament |
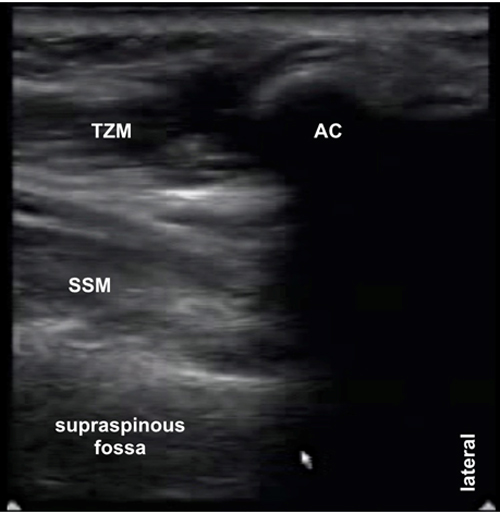
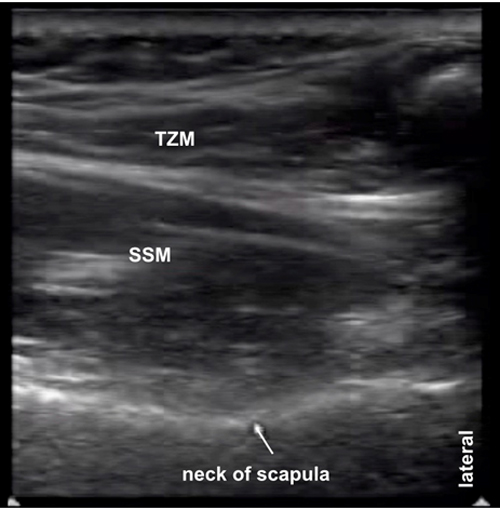
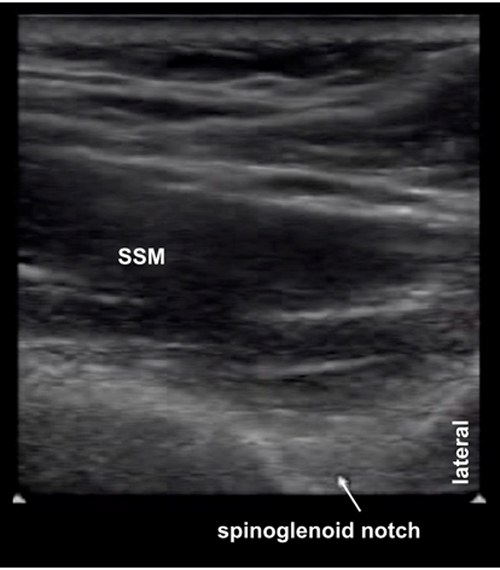
After traveling through the supraspinous fossa, the SSN reaches the spinoglenoid notch laterally and exits into the infraspinous fossa (Figure 3). Between the two notches, it is in direct contact with bone, covered by the inferior fascia of the supraspinatus muscle and accompanied by the suprascapular artery. The course of the SSN within the fossa is considerably oblique which has important impact on correct transducer positioning.
Figure 3. A schematic diagram showing superior view of the supraspinous fossa showing the course of the suprascapular nerve from the suprascapular notch to the spinoglenoid notch laterally
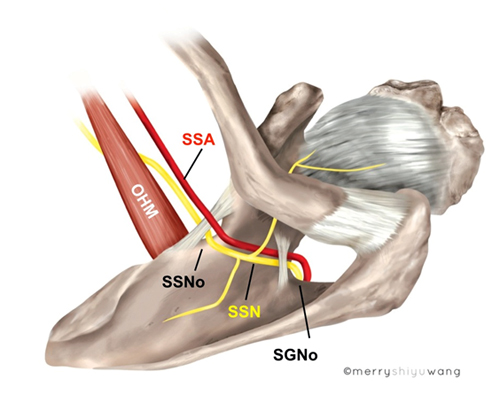 |
OHM = omohyoid muscle SGNo = spinoglenoid notch SSNo = suprascapular notch SSA = suprascapular artery SSN = suprascapular nerve |
The suprascapular nerve innervates the supraspinatus and infraspinatus muscles. It also provides sensory innervation to both the glenohumeral and acromioclavicular joints, the coracohumeral ligament, the subacromial bursa and the scapula.
From an anatomical perspective, it is best to block the nerve over the supraspinous fossa half way between the suprascapular notch and the spinoglenoid notch.
Movie 2.1. Suprascapular nerve anatomy