Scanning Technique
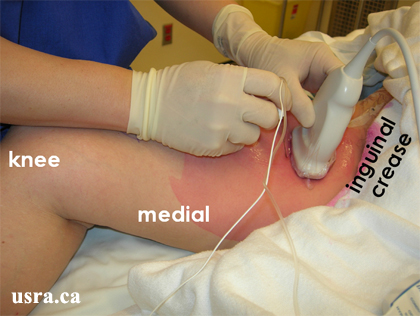
- Position the patient supine with the hip and knee slightly flexed and the hip externally rotated approximately 45 degrees.
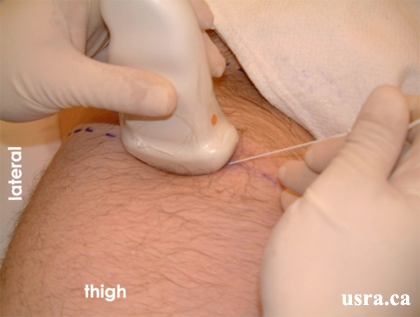
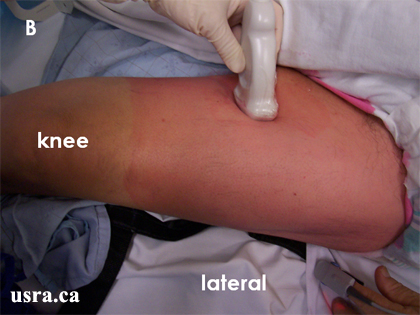
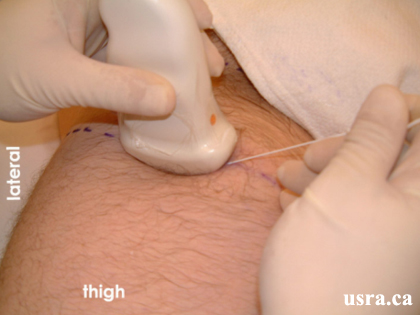
- After skin and transducer preparation (see transducer preparation section), place a curved low frequency 2-5 MHz transducer firmly on the thigh approximately 8 cm from the inguinal crease.
- Optimize machine imaging capability. Select appropriate depth of field (usually > 6 cm from the skin surface), focus range and gain. The skin to nerve distance is often greater than other sciatic nerve block approaches.
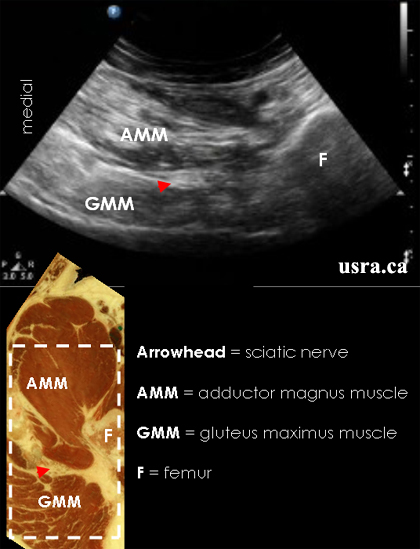
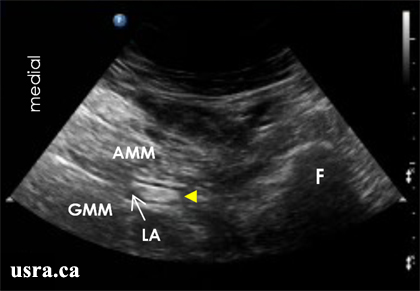
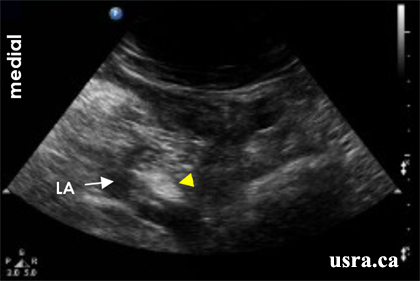
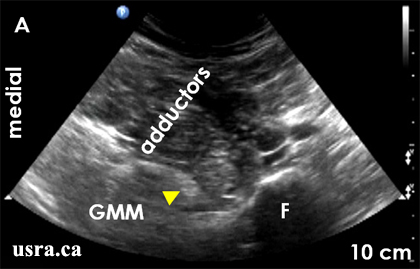
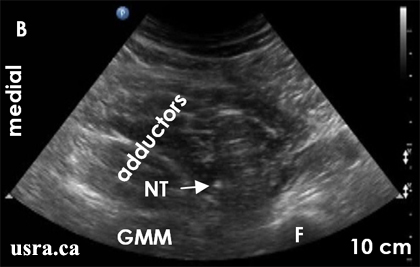
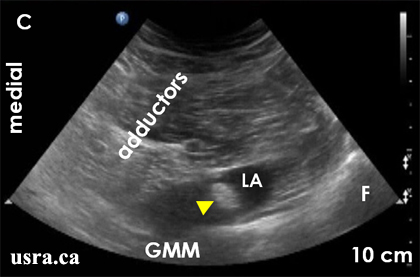
- Observe on the screen the transverse view of the femur and the sciatic nerve (short axis). The sciatic nerve in the proximal thigh appears predominantly hyperechoic (bright) and often oval or elliptical on ultrasound.
|
Transducer over the right proximal thigh, approximately 8 cm from the inguinal crease |