Clinical Pearls
Pitfalls in Nerve Localization
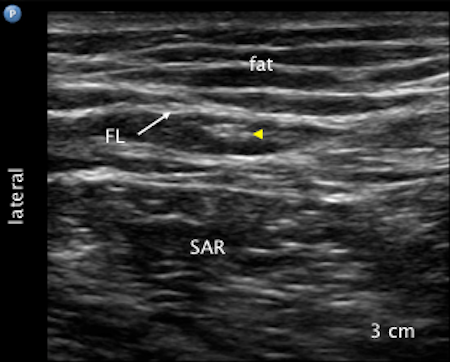
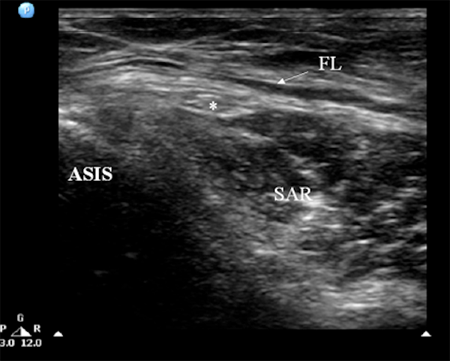
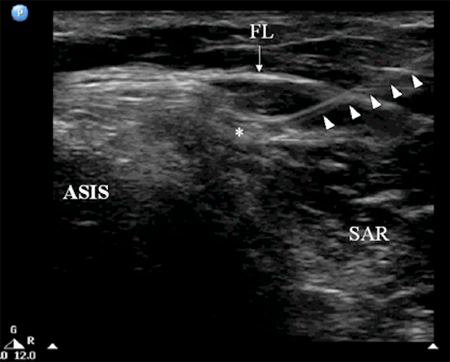
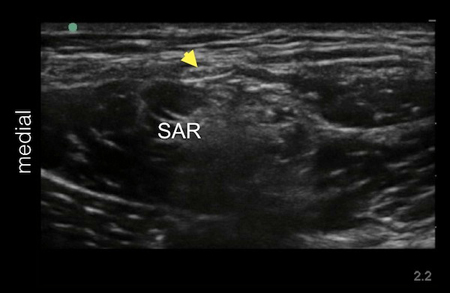
It is also common to visualize hyperechoic structures within the sartorius muscle.
It is important not to mistake the hyperechoic tendinous part of the sartorius muscle for the
LFCN. Differentiation is possible by performing a systematic dynamic scan to trace the
nerve in the fat filled space below the ASIS from distal to proximal and vice versa.
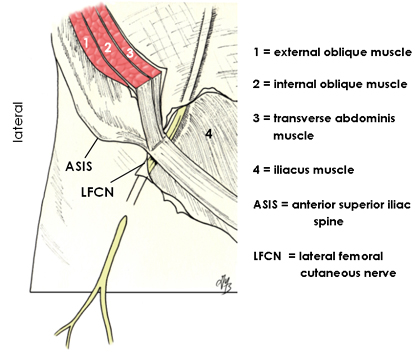
Course of the Lateral Femoral Cutaneous Nerve
The whole course of the LFCN as well as its formation is highly variable among individuals.
Thus the LFCN may not be found immediately medial to the ASIS. Other practical important
locations to locate the LFCN are:
- the nerve may be far more medially located, e.g., halfway between the ASIS and
the pubic symphysis or tubercle; in this case, the LFCN is sandwiched
between fascia lata and fascia iliaca before it comes on top of SM
- the nerve may course over the iliac crest lateral to the ASIS;
- very rarely, the LFCN runs through or deep to the substance of the sartorius
muscle (e.g., if the nerve is arising from the femoral nerve).
In these cases, tendinous part of the sartorius muscle may be mistaken
for the nerve.
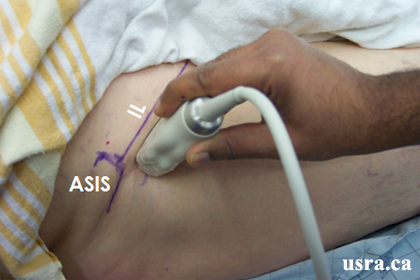
Note that regardless of anatomical variations, the key to success for locating the
LFCN is to first locate the nerve distally in the fat filled space and then trace
the nerve proximally towards the ASIS.
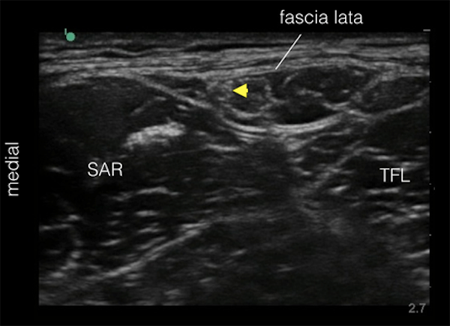
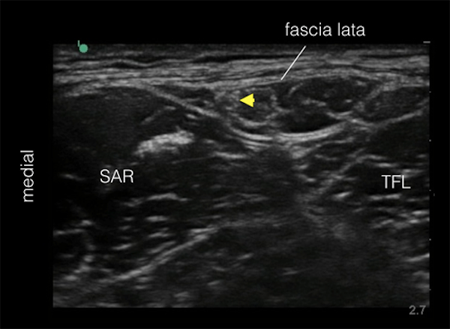
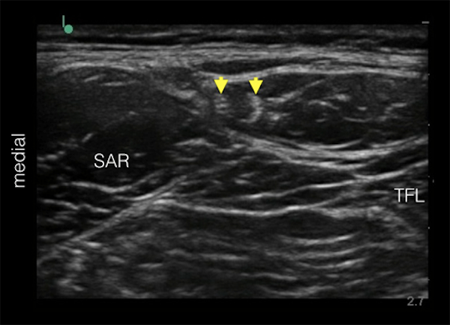
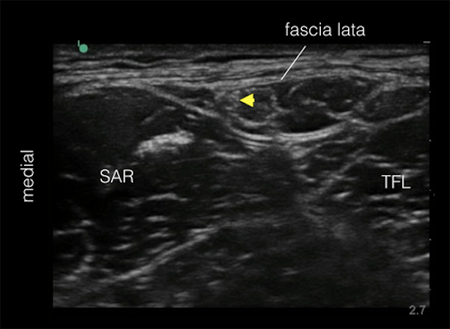
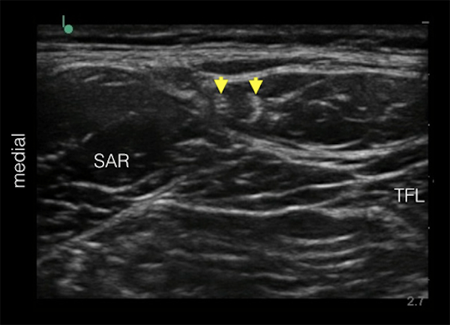
Nerve Located Between the Tensor Fascia Lata and Sartorius Muscles
The lateral femoral cutaneous nerve is usually visualized as a relatively hyperechoic nerve
structure in the proximal thigh (several cm inferior to the anterior superior iliac spine) within a
fat filled hypoechoic space. This space is found between the sartorius muscle medially and
the tensor fascia lata muscle laterally. The nerve is covered by the fascia lata, thus the
nerve is subfascial. Note that the nerve is not subcutaneous.